Classification of Nerve Injuries
Various classification systems have been developed to grade the severity of nerve injuries. These systems serve several important functions:
-
Facilitating communication among healthcare professionals
-
Supporting documentation of the injury
-
Advancing research in nerve injuries
-
Guiding prognosis and treatment plans
While these classifications may seem complex, the key concept to understand is that nerve injuries can range from mild to severe, and a single lesion can involve a mix of different severities.
Basic Anatomy
The basic building block of a nerve is a neuron which comprises a cell body and an axon. Axon may be myelinated or unmyelinated. Myelinated axons are surrounded by Schwann cells and a loose connective tissue called the endoneurium. A number of axons are collected into bundles called the fascicles which are covered by the perineurium. A number of fascicles are then grouped together to form a nerve which is surrounded by the epineurium.
Nerves have a rich segmental, longitudinal and interconnected blood supply.
Classification Systems
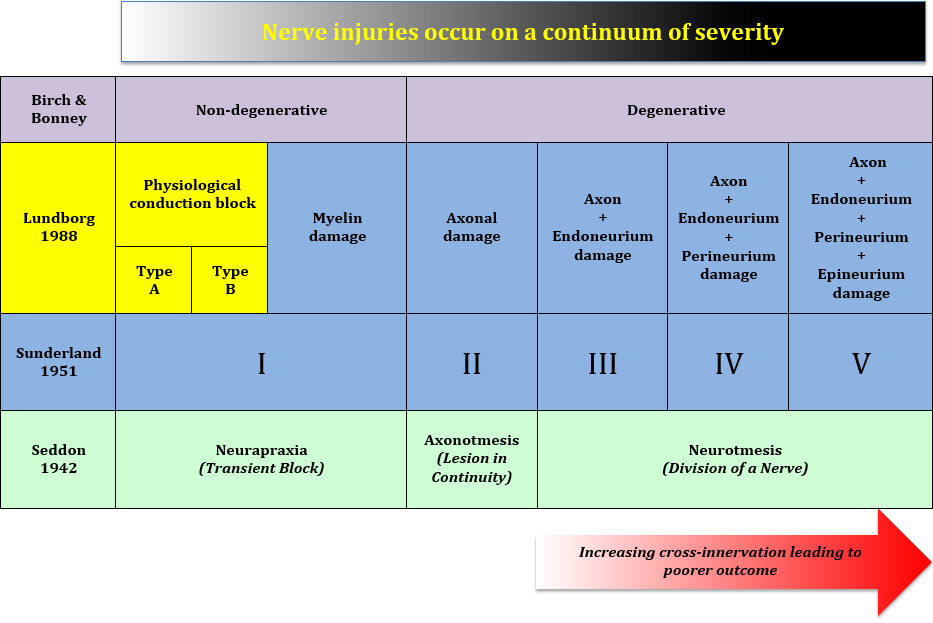
SEDDON CLASSIFICATION
The foundation of our current understanding of the classification of nerve injuries was laid down by Seddon, who was the Nuffield Professor of Orthopaedics, after studying some 460 nerve cases in Oxford. Seddon in fact proposed the classification in English (in brackets) initially but it was his colleague Henry Cohen, a prominent neurologist of the time, who suggested the use of Greek to avoid ambiguity!
-
Neurapraxia (Transient block)
-
This is the mildest form of nerve injury.
-
Providing the insult is removed in a timely manner, the prognosis is good and recovery is complete.
-
There is localised degeneration of the myelin sheath.
-
Axonotmesis (Lesion in continuity)
-
This is a more severe injury than neurapraxia.
-
There is complete interruption of axons and there is loss of conduction in the nerve fibre beyond the zone of injury.
-
Providing the insult is removed in a timely manner, the prognosis is still good and recovery can be complete.
-
There is preservation of supporting structures (Schwann tubes, endoneurium, perineurium).
-
Neurotmesis (Division of a nerve)
-
This is the most severe form of nerve injury.
-
If the nerve is completely transected, no recovery is possible unless it is surgically repaired.
-
The recovery can be unpredictable.
-
Histologically all essential parts are destroyed but interruption can occur without apparent loss of continuity.
SUNDERLAND CLASSIFICATION
Sunderland, who was the Professor of Anatomy and later Dean at Melbourne University did not like the use of Greek. He predicted that modern day doctors would not understand Greek. Instead, he proposed a numbered classification (I-V) that was based on incremental involvement of the various nerve sheaths after detailed investigation of the anatomy of peripheral nerves and long-term study of 300 cases of peripheral nerve injuries. He made reference to type I being equivalent to neurapraxia, but did not draw any further comparison to axonotmesis and neurotmesis.
With increasing severity of nerve injuries (III to V), there is greater disruption of nerve sheaths which could result in "cross-wiring" of the regenerating axons. This could lead to misinterpretation of signals which are being transmitted by the nerve to the brain as well as mis-firing of the wrong muscles.
LUNDBORG CLASSIFICATION
Lundborg, another giant in nerve surgery, proposed the concept of physiological conduction block to help us understand the wide range of clinical behaviours in seemingly innocuous insults to the nerves.
-
Type A
-
The insult has caused intraneural circulatory arrest.
-
This is a form of metabolic block with no nerve fibre pathology.
-
It is immediately reversible (as the insult is transient).
-
Type B
-
There has been greater degree of insult to the nerve such that there is intraneural oedema.
-
There is increased endoneurial fluid pressure.
-
It is reversible within days or weeks (after removal of the insult).
BIRCH & BONNEY CLASSIFICATION
In the UK, Birch & Bonney, who have made significant contribution to our understanding of nerve injuries, proposed a pragmatic distinction between a non-degenerative and a degenerative nerve lesion. In the latter, there is Wallerian degeneration of the nerve fibre.
MIXED INJURY
It is however important to appreciate that any nerve injury is often mixed and there could be a spectrum of severity in any segment of lesion. This observation was made by the various pioneers in nerve surgery but it was Mackinnon and Dellon who coined the term Sunderland ‘VI’ in order to capture this important concept.